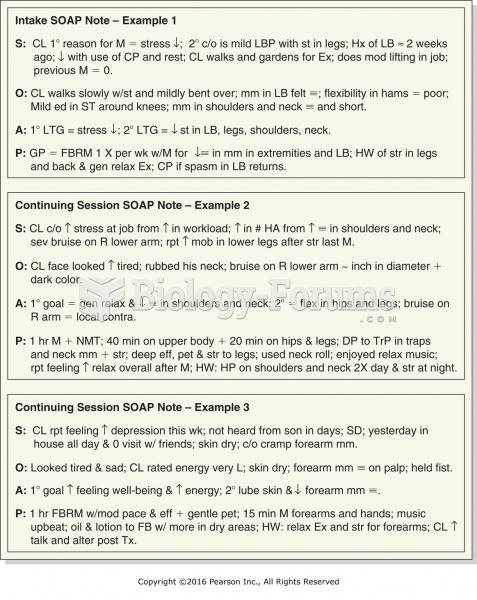
The P in SOAP note stands for:
a. plan.
b. purpose.
c. patient.
d. proposed.
(
Q. 2) The portion of the SOAP note that contains what the physician sees, hears, feels, and so on is the:
a. Subjective.
b. Objective.
c. Assessment.
d. Plan.
(
Q. 3) To save space on a page the writer can do any of the following EXCEPT:
a. continue onto another page.
b. use both sides of the page.
c. use approved abbreviations.
d. write in the margins.
(
Q. 4) Where would information related to the physicians referral for a CT scan be located in a SOAP note?
a. S
b. O
c. A
d. P
(
Q. 5) Where would the information obtained from a child's parent be noted in a SOAP note?
a. S
b. O
c. A
d. P
(
Q. 6) Diagnostic possibilities that the physician is considering would be found in which part of a SOAP note?
a. S
b. O
c. A
d. P
(
Q. 7) Instead of trying to correct information in a medical record:
a. place a sticky note over the erroneous information.
b. white-out the error and write in the correction.
c. write an addendum that describes the error and the correct information.
d. do nothing.
(
Q. 8) The most common note format is the:
a. SOAP notes.
b. POMR notes.
c. SAOP notes.
d. PMRO notes.
(
Q. 9) When making a notation in the medical record, which of the following is NOT necessary?
a. Date of the entry
b. Information you are documenting
c. Signature of the writer
d. Initials of the writer
(
Q. 10) Why does the patient name NOT appear on the outside of the medical record?
a. It is unsightly.
b. It is the law.
c. It protects patient confidentiality.
d. It allows for easier filing.
 Quick Reply
Quick Reply