What symptoms might result from hypernatremia ("high blood-sodium" level)?
Osmotic shrinkage of cells during hypernatremia can cause shrinking of the brain and concomitant central nervous system symptoms such as lethargy, confusion, coma, convulsions, and respiratory paralysis. Muscular tremor, rigidity, and hyperreflexia may also occur.
How is this patient's interstitial edema in the lungs affected by his already-weakened heart?
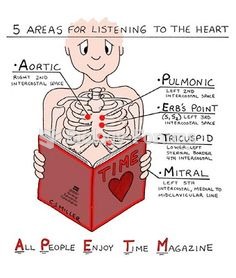
This process is exacerbated by the patient's underlying chronic renal failure and heart attack. His failing kidneys have a difficult time excreting the excess sodium and chloride ions introduced into his body. Furthermore, his recent heart attack places him at increased risk of developing congestive heart failure. His left coronary artery blockage probably caused damage to his left ventricle. The osmotic increase in blood volume places an increased pre-load work requirement on an already impaired left ventricle. If this ventricle cannot pump blood out into the aorta at a rate equal to that of blood entering the left ventricle from the left atrium, hydrostatic pressure will rise in the left ventricle, left atrium, and ultimately the pulmonary circulation "upstream." An increase in pulmonary capillary hydrostatic pressure will force more water to be filtered from the bloodstream into the interstitial spaces of the lung tissue. As fluid builds up in these spaces, it may begin to collect in the alveolar air spaces and terminal bronchioles (a condition called "pulmonary edema"). If this happens, rales (i.e. crackling sounds) may be heard with a stethoscope when the patient inhales. These are the sounds of obstructed airways "popping open."
 Quick Reply
Quick Reply