|
Answer to #1
Sodium (low): Edema; hemodilution
PO4 (high): Retention and release of P from bone breakdown
GFR (low): Reflection of decreasing renal function
PT/INR (high): Reflection of anticoagulants given for dialysis
BUN (high): Retention
Creatinine (high): Retention
Calcium (low): Decreased active vitamin D/edema
Anion gap (low): Acidosis and/or electrolyte imbalance
Total protein, albumin (low): Value most likely skewed by edema
Hemoglobin, hematocrit, MCV, MCH, MCHC, RBC (low): anemia secondary to renal failure/decreased erythropoietin
Transferrin (low): decreased due to nephropathy
Ferritin (low): Edema/hemodilution
Answer to #2
Glomerulonephritis is inflammation of the nephrons (specifically the glomerular capillary loops). There can be multiple causes including infections such as Streptococcus; complications from chronic diseases such as lupus, diabetes, or high blood pressure; or vasculitis. The loss of nephron function results in an inability to filter blood appropriately, leading to azotemia.
Answer to #3
The body down-regulates albumin synthesis so that needed positive acute-phase proteins for the immune system (antibodies, complement, cytokines, C-reactive protein), clotting (fibrinogen), and wound healing can be made.
Production of cytokines such as IL-1, IL-6, and tumor necrosis factor (TNF) is increased, which alters hormone secretion to favor a catabolic state, increasing muscle catabolism, gluconeogenesis, and lipolysis. These cytokines also inhibit protein synthesis (albumin, prealbumin, transferrin, retinol-binding protein) and muscle repair.
Extracellular fluid is expanded (due to edema), causing biochemical tests to be diluted and results to appear low.
Resting energy expenditure is elevated/increased and protein requirements are increased, making energy and protein needs difficult to accurately determine.
If the cause of metabolic stress is severe or prolonged, nutrition intervention alone will not prevent muscle protein loss in inflammation if nutritional intake is inadequate. Therefore, measurement of albumin/ prealbumin is not an accurate measure for diagnosis of malnutrition when inflammation is present.
Answer to #4
ICD-10 Diagnosis Code E40 - Kwashiorkor
Severe malnutrition with nutritional oedema with dyspigmentation of skin and hair.
ICD-10 Diagnosis Code E41 - Nutritional marasmus
Severe malnutrition with marasmus. (energy depletion/ reduced fat stores out of proportion with lean body mass loss)
ICD-10 Diagnosis Code E42 - Marasmic kwashiorkor
Severe protein-energy malnutrition
- Intermediate form
- Signs of kwashiorkor and marasmus
ICD-10 Diagnosis Code E43 - Unspecified severe protein-energy malnutrition
Severe loss of weight wasting in children or adults, or lack of weight gain in children leading to an observed weight that is at least 3 standard deviations below the mean value for the reference population (or a similar loss expressed through other statistical approaches). When only one measurement is available, there is a high probability of severe wasting when the observed weight is 3 or more standard deviations below the mean of the reference population.
ICD-10 Diagnosis Code E44 - Protein-energy malnutrition of moderate and mild degree
Weight loss in adults/children (or the lack of weight gain in children) that is 1 to 3 standard deviations from the reference population.
ICD-10 Diagnosis Code E45 - Retarded development following protein energy malnutrition
Short stature, stunting, or physical retardation related to malnutrition
ICD-10 Diagnosis Code E46 - Unspecified protein-energy malnutrition
Malnutrition or protein-energy imbalance that is not specified otherwise.
Answer to #5
The kidneys maintain homeostatic balance in the body through 3 basic functions:
Filtration: Continuous filtration of blood removes waste products and fluid
Blood pressure control:
Specialized cells (of the glomerulus) in the kidneys secrete renin to form angiotensin I
Angiotensin I is converted to angiotensin II, a powerful vasoconstrictor
Angiotensin II also stimulates production of aldosterone and control of blood pressure
Hormone production:
Kidneys produce erythropoietin, a hormone responsible for red blood cell production in bone marrow
Active form of vitamin D is also produced by the kidneys, allowing calcium to be absorbed
Answer to #6
Malnutrition associated with chronic disease - this includes chronic diseases or conditions that have sustained mild to moderate inflammation (organ failure, pancreatic cancer, rheumatoid arthritis, diabetes mellitus, metabolic syndrome, chronic kidney disease, etc.)
Loss in lean body mass is gradual and can eventually reach significant depletion over time (several months). With nutritional intervention, lean body mass loss is slowed or potentially reversed.
Positive response to nutrition intervention also requires successful medical treatment of underlying disease.
Malnutrition associated with acute illness and inflammation - this includes acute diseases or injury states with acute and severe inflammatory responses (major infection, burns, trauma, or closed head injury)
Significant depletion of lean body mass occurs over a short period of time (<1 month) without nutritional intervention. there are persistent signs of inflammation. with intervention, lean body mass loss is slowed, but still occurs if inflammation persists.
Priority of nutrition intervention is to provide nutrients to support organ system function and preserve immune function while acute medical treatment is provided.
Answer to #7
Date, Time; Nutrition Note
A: 24 yo Native American female, ht 5'0; wt. 77.2 kg; aBWef 70 kg
Dx: chronic kidney disease on hemodialysis; type 2 DM. Meds: Glucophage, captopril
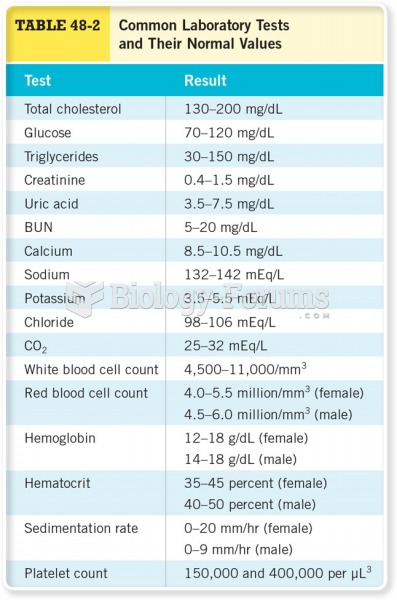
Labs: Na 130; K 5.8; Cl 91; CO232; HCO3 22; BUN 69; Cr 12; Glu 282; Hgb A1C 9,2; PO46.4; Ca 8.2; Alb 3.3; Hgb 10.5.
D:
Inadequate protein-energy intake related to recent poor appetite and nausea and vomiting secondary to CKD as evidenced by typical recent daily intake of 1300 kcal and 64 g protein compared to recommended 2450 kcal and 72 g protein (hemodialysis)
Limited adherence to nutrition-related recommendations as evidenced by patient stating that she tried to follow the diet that she was taught 2 years ago but it was hard to keep up
Undesirable food choices as evidenced by consumption of higher-sodium foods such as processed meats, potato chips, and crackers
I:
Patient Goals:
Nutrition prescription: Diet Rx: 35 kcal/kg (2450 kcal/day), 1.2 g protein/kg (72 g/day), 2 g K, 1 g phosphorus, 2 g Na, 1,000 mL fluid + urine output per day.
Normalization of BG and A1c
Decrease intake of foods high in sodium
Patient able to sustain changes in diet based on recommendations for dialysis
Intervention: Provided counseling that included purpose of dietary changes consistent with nutritional consequences of chronic kidney disease and treatment with dialysis; assessed readiness and self-efficacy for change. Strategies included motivational interviewing, self-monitoring, and problem solving. Provided detailed list of foods that are high in sodium with alternatives to improve taste. Patient also provided with instructions for recording food intake and BG.
M: Patient able to identify the relationship between dietary intake and renal function. Monitor weight status, hydration status, electrolytes (K, P, Na, Ca), glucose, and anemia pertinent values (Hct, Hgb, RBC). Expressed desire to sustain changes over time and acknowledged that family is supportive of nutrition and medical care. Plan to see daily while in hospital and schedule outpatient within two weeks of discharge. Referral to dialysis RD once treatment scheduled.
Answer to #8
inadequate nutrient supply
decrease in basal metabolic rate to conserve energy (decreased thyroid function leads to decreased BMR)
liver glycogen stores used up in first 12-24 hours (glycogenolysis)
energy from fat storage (lipolysis) provides >90 of kcal (ketones as primary energy source)
energy from protein/lean mass provides <10 of kcal for gluconeogenesis to provide glucose for obligate users (brain)
increased need for alanine and glutamine (from muscle) to stimulate gluconeogenesis
protein losses significant during first 7-10 days (1-2 kg lean body mass lost over first 7 days; skeletal muscle catabolized, muscle synthesis decreased)
organ function changes in GI tract result in loss of mass, decreases in villi, decreased enzyme secretion, impaired motility, and bacterial overgrowth, which lead to maldigestion and malabsorption
decreased protein synthesis in liver
muscle function decreases; breakdown of intercostal muscles can lead to decreased respiratory function; breakdown of cardiac muscle can lead to hypotension, bradycardia, and decreased cardiac output
immune function decreases to spare protein
decreased growth
|
 Quick Reply
Quick Reply