|
Answer to #1
Fibromyalgia, also referred to as fibromyalgia syndrome or FMS, is a chronic musculoskeletal disorder characterized by widespread muscle pain, joint stiffness, disturbed sleep, fatigue, headache, cognitive and memory problems (sometimes referred to as fibro fog), paresthesias, irritable bowel syndrome, painful menstrual periods, and numerous tender points, which are specific muscle-tendon sites throughout the body that are painful when pressed. Fibromyalgia is the second most common musculoskeletal condition encountered by rheumatologists, affecting an estimated 5 million adults in 2005 . Prevalence is about 2, and is much higher among women than men (3.4 vs. 0.5). The etiology of fibromyalgia is multifactorial and includes both environmental and genetic factors. Treating fibromyalgia involves a multidisciplinary approach aimed at improving the quality of sleep; treating depression, anxiety, and pain; increasing physical activity; and using various approaches to help patients better cope with stressful events and improve their ability to relax.
Answer to #2
d
Answer to #3
Persons 65 years old and older are at increased risk of osteomalacia due to diets low in calcium and vitamin D, a lack of sun exposure, decreased efficiency in synthesizing vitamin D, and increased incidence of intestinal malabsorption problems. The treatment of osteomalacia should address the underlying causes. Effective treatment of vitamin D deficiency may require a multivitamin providing as much as 20 g of vitamin D. Calcium intake should be adequate and may require a supplement providing as much as 1,5002,000 mg of elemental calcium per day. Patients with severe, longstanding vitamin D deficiency may initially require pharmacologic doses of up to 1,250 g per week for 312 weeks, followed by maintenance therapy of 20 g per day. Patients taking drugs that accelerate hepatic breakdown of vitamin D, and those with intestinal malabsorption problems, will require vitamin D in doses much greater than the RDA. Patients with liver or kidney diseases that prevent the activation of vitamin D into its biologically active form will require a form of vitamin D that is already biologically active, such as calcitriol.
Answer to #4
c
Answer to #5
Risk of osteoporosis (primary or secondary) and related fractures is influenced by a number of factors. Risk factors having a particularly strong bearing on the development of peak bone mineral density from childhood through early adulthood include genetic susceptibility and family history, female sex, Caucasian race, premenopausal amenorrhea, physical inactivity, and low lifetime calcium and vitamin D intakes. Low lifetime intakes of fluoride, magnesium, and zinc may also have a bearing. Genetics is a particularly important determinant of peak bone mass and of subsequent fracture risk. Factors that decrease bone remineralization and/or increase demineralization once peak BMD has been achieved include female sex, premenopausal amenorrhea, menopause before age 45 years, age, glucocorticoid therapy, cigarette smoking, physical inactivity, and low intakes of calcium and vitamin D. Low intakes of fluoride, magnesium, zinc, and vitamin K may also influence bone demineralization.
Answer to #6
a
Answer to #7
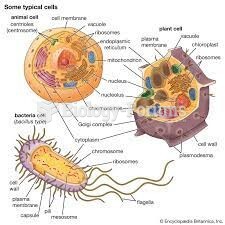
Osteoblasts, or bone-building cells, produce the ECM and then participate in the calcification or mineralization of the matrix, in a process known as bone formation or mineral deposition. Active osteoblasts are found on the surface of newly forming bone. They remove ions of calcium, phosphate, and other minerals from the blood plasma and deposit them within the bone ECM, thus hardening it. In response to bone fracture or the stress of weight-bearing exercise, the osteogenic cells multiply more rapidly and then differentiate to become osteoblasts.
|
 Quick Reply
Quick Reply